Alzheimer’s disease is a chronic progressive generalized degeneration of nervous system cells which causes gradual mental capability deterioration. It was named after Dr. Alois Alzheimer who first described the disease. It is the most common form of dementia. Dementia is a broad term for memory loss and cognitive impairment. There is currently no curative treatments for Alzheimer’s disease. However, there are some treatments which can slow down the progress of disease. It is associated with Lewy body dementia.
Epidemiology
- Age: The majority of people affected by Alzheimer’s disease are 65 years or older.
- Gender: Females are more commonly affected; with a male to female ratio of around 1:2.
- Most commonly seen in Western Europe and the USA.
- Accounts for 60-80% of all dementia cases worldwide.
Types
There are two broad types of Alzheimer’s based on probable etiology of the disease-
- Inherited
- Sporadic
- Inherited Alzheimer’s disease occurs in 5-10% of cases. It is an autosomal dominant variety of disease and manifests earlier in life at around 35-45 years. Commonly caused by a mutation in the APP (Amyloid Precursor Protein) gene, PSEN-1 (Presenilin-1) gene, and PSEN-2 (Presenilin-2) gene.
- People with Down syndrome are at higher risk of developing Alzheimer’s disease because in Down syndrome there is an extra copy of chromosome 21. The APP gene is located in chromosome 21 and therefore there is an extra copy of the APP gene.
- Sporadic Alzheimer’s disease is the most common form of this disease occurring in 90-95% of cases. The disease typically manifests later in life at above 65 years of age. Various risk factors described below seem to play a role.
Risk factors
- Advancing age
- Genetics (APOE e4 gene)
- Dyslipidemia
- Alcohol
- Hypertension
- Insulin resistance
- Obesity
- Depression
- Antisocial personality
- Infection
- Stroke
- Delirium
- Traumatic injury of the brain
Pathophysiology
- Pathological processes in Alzheimer’s disease start 10-15 years prior to disease manifestation.
- Alzheimer’s disease primarily targets the cerebral cortex and hippocampus.
- The temporal lobe and parietal lobes of the cerebral cortex are first affected resulting in memory problems and spatial navigation problems.
- The exact mechanism of Alzheimer’s disease is yet to be established.
- Researchers have focused on a few hypotheses contributing to the development of Alzheimer’s disease.
Tangle formation-
- In healthy neurons, the internal support structures are made of microtubules that carry nutrients and other substances along the length of neurons.
- These microtubules are bound together by a special kind of protein called ‘tau’.
- In Alzheimer’s disease, the tau proteins start to bind among themselves, forming neurofibrillary tangles and leaving the microtubules unsupported.
- The microtubules thus begin to collapse.
- These neurons undergo apoptosis.
Plaque deposition-
- Amyloid Precursor Protein (APP) is present in neuronal cell membranes.
- It helps neuron growth and repair.
- Normally, the APP gets broken down by enzymes and the broken-down products are soluble, which is degraded by the body.
- In Alzheimer’s disease, the APP is broken down into abnormal insoluble fragments called beta-amyloid.
- Beta amyloids together form plaques and deposit between neurons.
- Disrupts neuron signaling pathway causing impaired memory.
- These plaques might also cause inflammation that damages the neurons.
Reduced choline acetyltransferase production-
- Causes reduced Acetylcholine (Ach) synthesis
- Reduced signaling in the cerebral cortex
Excessive activation of NMDA receptors-
- Promotes cell death
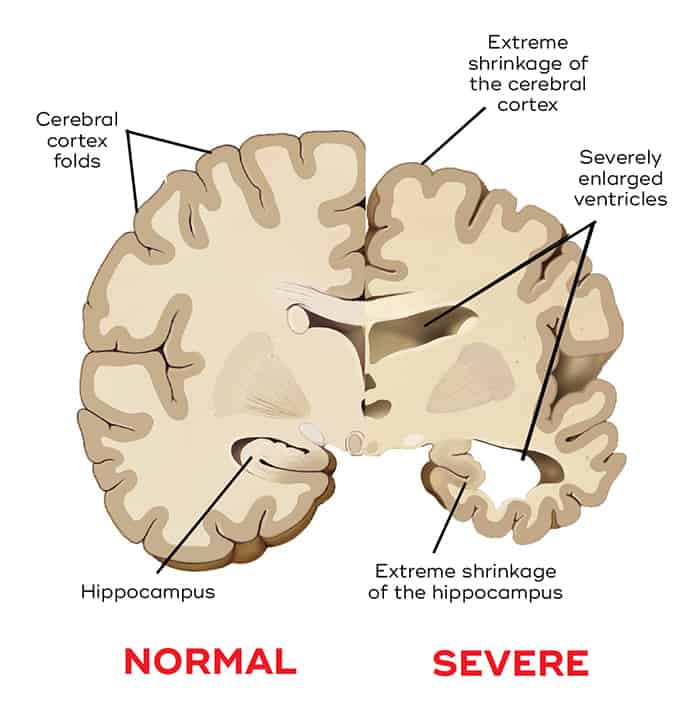
Changes in the brain
Macroscopic changes-
- Brain atrophy
- Narrow zyrus
- Wider sulci
- Larger ventricles
Microscopic changes-
- Loss of neurons
- Neurofibrillary tangles
- Plaques
Biochemical changes-
- Type-A beta amyloid deposition in cortex
- Deficiency of acetylcholine
Alzheimer's symptoms
Memory impairment
- Forget dates or appointments
- Repetition of questions or sentences
- Getting lost in familiar places
- Forgetting personal details
- Misplacing objects
- Eventually forgetting family members
Behavioral and psychological symptoms-
- Apathy
- Depression
- Anxiety
- Irritability
- Aggression
- Loss of inhibition
- Loss of trust
- Social withdrawal
- Delusion
Difficulty in concentrating-
- Starts with difficulty in multitasking
- Later on, progresses to loss of concentration in a single task
- Loss of basic skills (such as- dressing, self-feeding)
Impaired thinking and reasoning
Alzheimer's disease stages
Stage | Characteristic | Symptom |
Stage-1 | Asymptomatic. Positive family history may raise concern. | None |
Stage-2 | Very minor symptoms start to appear. | Forgetfulness |
Stage-3 | Mild impairment of mental function may be noticed by very close persons. | Poor concentration Reduced memory Difficulty finding the right word during the conversation |
Stage-4 | Clearcut disease symptoms start to show up. | Short term memory loss May forget important details about life May forget to pay bills |
Stage-5 | Impairment in daily activities due to significant confusion. Needs help from friends or family members. | Inability to recall simple details about oneself Difficulty in getting dressed |
Stage-6 | Severe form of disease. Required professional support. | Unaware of the surrounding environment Inability to recognize faces Behavior and personality changes Loss of bladder and bowel control |
Stage-7 | Most severe and final stage of the disease. | Loss of speech Loss of facial expression Does not respond or communicate Wandering |
For the purpose of treatment modality, some experts simply group it into-
- Early disease (mild)
- Moderate disease (moderate)
- End disease (severe)
Diagnosis
Alzheimer’s disease may be diagnosed using the list of criteria laid out by NINCDS-ADRDA (National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association). This criterion takes into account the complaints presented by the patient, other medical illnesses, and a neuropsychological evaluation.
Criteria for diagnosing Alzheimer’s disease-
- Definite Alzheimer’s disease: Histopathological features of Alzheimer’s in autopsy or brain biopsy
- Probable Alzheimer’s disease: Dementia established by clinical and neuropsychological examination + progressive cognitive impairment in more than one areas of cognition + onset of symptoms at age between 40 to 90 + no disturbance in consciousness + absence of other causes of dementia
- Possible Alzheimer’s disease: Dementia symptoms present with an atypical presentation, onset or clinical course + progressive deficit in a single area of cognition + no other causes of dementia is found
- Unlikely Alzheimer’s disease: Sudden onset dementia symptoms with focal neurological signs
Neuropsychological evaluation
- Mini-Mental State Examination (MMSE): ≤ 24 suggests dementia
Investigations
- MRI- Widening of lateral ventricles, cerebral cortical atrophy
- CT Scan- to rule out tumor, stroke, head injury
- PET Scan- to identify the pattern of degeneration
- Blood test- for genetic testing, electrolytes, vitamins, and thyroid.
Treatment
There is no cure for Alzheimer’s disease. But there are certain medications, therapies, and lifestyle changes to ease the symptoms and slow down the disease progression.
Medication
Medications for cognitive symptoms-
- Donepezil, Rivastigmine, and Galantamine (Acetylcholinesterase inhibitors)-
- Helps to retain memory. Used in mild to moderate disease, but may be used in late stages as well.
- Side effects- nausea, vomiting, diarrhea, heart block (A-V block), bradycardia, insomnia
- Donepezil, Rivastigmine, and Galantamine (Acetylcholinesterase inhibitors)-
- Memantine (NMDA receptor antagonist)
- Used in moderate to severe disease or in those who cannot tolerate Acetylcholinesterase inhibitors
- Side effects- diarrhoea, constipation, cough, dizziness, confusion.
Medicines to treat behavioral changes
- Antipsychotics- haloperidol, clozapine, risperidone, etc.
- Antidepressants- citalopram, fluoxetine, sertraline, etc.
- Anxiolytics- lorazepam, oxazepam etc.
Therapies
- Cognitive stimulation therapy- exercise to improve memory and problem-solving ability.
- Cognitive rehabilitation- personal goal-oriented training to improve skills.
- Reminiscence- talking about events of past.
- Life story work- a compilation of photos and notes from childhood till the present time.
Lifestyle measures
- Getting enough rest
- Stay calm
- Limit confusion
- Focus on one task at a time
Prevention
Prognosis
- Symptoms always worsen over time, but the rate varies.
- Early-onset Alzheimer’s disease tends to show a more rapid and aggressive course than late-onset disease.
- The survival period varies from 3 to 20 years after diagnosis.
- Death primarily occurs due to infection, like pneumonia.